






















 ChatGPT
ChatGPT
A healthcare CRM is a purpose-built patient relationship management system designed to handle HIPAA-regulated data, integrate with EHR platforms, and automate the clinical and administrative workflows that generic CRM tools were never designed for. Pick the wrong one and you inherit either a compliance liability or a system that can’t talk to your EHR. The choice comes down to three variables: your integration requirements, your data ownership needs, and whether your patient workflows are standard enough for an off-the-shelf product or complex enough to justify a custom build.
Most healthcare organizations already know they need one. What they don’t know is what building one actually involves, and that gap is where projects go wrong. Timelines blow out because EHR sandbox access takes longer than anyone planned. Budgets collapsed because HIPAA architecture was scoped as an afterthought. And vendors get selected without anyone asking the one question that determines legal liability from day one.
Deborah Vick is the CEO of Vicktorious Academy and a chronic illness patient advocate who has navigated complex healthcare systems across nearly 40 years of personal experience with multiple chronic illnesses, both visible and invisible. Her perspective on where communication breaks down is direct:
That’s the problem a well-built healthcare CRM solves. This guide covers what it takes to build one properly.
TL;DR
- A healthcare CRM manages the relationship layer; communication history, follow-ups, referral tracking, while your EHR handles the clinical record. They’re complementary, not interchangeable.
- Generic CRMs (Salesforce, HubSpot) aren’t built for PHI. Retrofitting HIPAA compliance onto one almost always costs more than building right from the start.
- Before you sign any dev partner: ask if they’ll sign a Business Associate Agreement (BAA). If there’s hesitation, walk away, it’s a legal requirement, not a formality.
- Realistic build costs: MVP $40K–$80K · Mid-market $80K–$150K · Enterprise $150K–$300K+. The single biggest variable is EHR integration.
- EHR credentialing (Epic, Cerner) takes 6–12+ weeks before a line of integration code can be written. Any timeline that doesn’t account for this will slip.
- HIPAA compliance is a foundation, not a feature. Scoping it as a late-stage checklist is the #1 source of cost overruns.
- Budget 15–20% of your build cost annually for maintenance, security patches, and EHR API updates.
- Off-the-shelf SaaS works if you have fewer than 20 users and standard workflows. Custom makes sense when you need deep EHR interoperability, full data ownership, or a platform that scales with your org.
What Is Healthcare CRM Software, And How Is It Different from a Regular CRM?
Your EHR stores diagnoses, prescriptions, lab results, and encounter notes. It’s a clinical record, built to support treatment decisions and regulatory documentation. A healthcare CRM manages a different layer entirely: who contacted the patient and when, whether they showed up to their follow-up, which referral source sent them, and how they’re engaging with their care plan between visits.
The two systems are complementary. They’re meant to talk to each other. But they’re not interchangeable, and confusing them is exactly how healthcare organizations end up building the wrong thing.
A regular CRM, Salesforce, HubSpot, Zoho, handles leads, deals, and contacts. That architecture simply doesn’t map to healthcare. There’s no concept of Protected Health Information (PHI) in a standard CRM schema. There’s no HIPAA audit log. Role-based access doesn’t account for clinical roles. And the moment a developer working on your CRM touches real patient data in a test environment, you’ve created HIPAA exposure that a standard software vendor agreement doesn’t cover.
A purpose-built healthcare CRM solves for all of this from the ground up, with a data model that treats patient identity, consent, and communication history as first-class objects, and with a compliance architecture that’s built in, not bolted on.
The distinction matters practically. Organizations that start with a generic CRM and try to ‘add HIPAA compliance‘ later almost always discover the same thing: the architectural debt is too deep to fix incrementally. It’s cheaper, and faster, to build right from the start, which is exactly what purpose-built healthcare software development is designed to do.
EHR vs. Healthcare CRM: Key Differences
| Function | EHR (Electronic Health Record) | Healthcare CRM |
|---|---|---|
| Primary purpose | Store and manage clinical data | Manage patient relationships and communication |
| Data it holds | Diagnoses, prescriptions, lab results, encounter notes | Communication history, engagement records, referral sources, care plan adherence |
| Patient outreach | Limited: portal messages only | Multichannel: SMS, email, telephony, automated sequences |
| Analytics | Clinical outcomes and documentation metrics | Engagement rates, communication effectiveness, referral attribution |
| Regulatory requirement | HIPAA, ONC certification | HIPAA compliance (BAA required with vendor) |
Why Healthcare Organizations Are Prioritizing Custom CRM Right Now
The short answer is that off-the-shelf tools have hit a ceiling, and patients have started noticing.
Patient volumes are climbing. Chronic disease management requires more touchpoints than any manual workflow can sustain. Telehealth’s permanence has multiplied the number of communication channels healthcare organizations are expected to manage simultaneously.
But the deeper pressure is something Deborah Vick articulates from the patient side with precision. She has spent decades managing multiple chronic conditions across fragmented provider networks, and she describes the structural communication failure that no amount of portal technology has fully solved:
One of the biggest challenges is the lack of interoperability between healthcare systems. I currently receive care from specialists across multiple healthcare organizations. While some information is shared, critical clinical notes, provider observations, and treatment rationale are often missing. This means patients must repeatedly tell their stories, explain complex medical histories, and bridge communication gaps between providers. During hospitalizations or urgent medical situations, these gaps can delay care and create unnecessary confusion. — Deborah Vick, CEO, Vicktorious Academy
Referral leakage is a growing problem for hospital networks: patients referred to a specialist and never followed up represent both a care gap and lost revenue. Automated referral tracking, a core CRM function, can recover significant volume that simply disappears in organizations still running on spreadsheets and manual follow-up calls.
The practices and health systems investing in CRM infrastructure are recognizing something straightforward: the relationship layer of healthcare has always existed. What’s changed is that patients now have enough options to punish organizations that manage it poorly.
Vick also illustrates what effective healthcare communication actually looks like in practice, and what makes it possible sharing her perosnal experience:
That kind of interaction, a provider who can pull communication history, review the chart, and make a real-time clinical decision without an in-person visit, is exactly what a well-integrated healthcare CRM infrastructure makes possible at scale.
The practices and health systems investing in CRM infrastructure are recognizing something straightforward: the relationship layer of healthcare has always existed. What’s changed is that patients now have enough options to punish organizations that manage it poorly. The broader forces driving this shift, value-based care, AI-assisted workflows, interoperability mandates, are covered in depth in our healthcare software development trends roundup, if you want the fuller picture of where healthcare technology investment is heading in 2026.
Core Features of a Healthcare CRM System
Not every healthcare CRM needs every capability on this list. The right feature set depends on your org type, patient volume, and integration landscape. But these are the modules that appear in most production-grade systems.
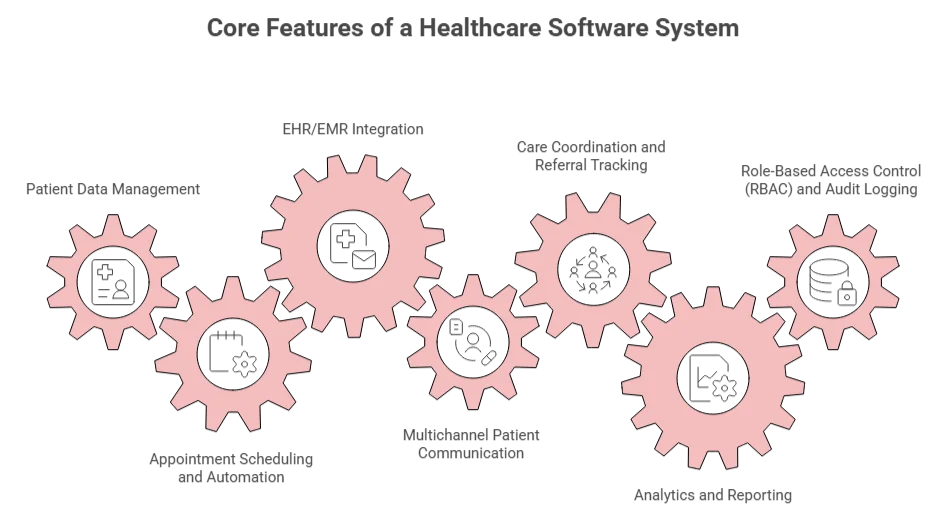
Patient Data Management
It is the foundation. A healthcare CRM needs a unified patient record that pulls from multiple sources, your EHR, scheduling system, and billing platform, and presents a coherent view without duplicating data. This requires careful data modeling to handle patient identity matching, consent tracking, and PHI tagging so the system knows which fields require encrypted storage and access controls.
Vick identifies a specific dimension of patient data that most system designers miss: the gap between clinical documentation and lived reality.
Building in structured mechanisms for patients to flag discrepancies in their records, and for those flags to reach the right person, is a design decision, not an afterthought.
Appointment Scheduling and Automation
Automated reminders via SMS, email, and voice. Rescheduling workflows. No-show follow-up sequences. This module alone can materially move metrics, studies consistently show automated reminders reduce no-show rates by 20–40%, which at scale represents significant recovered revenue.
EHR/EMR Integration
It is the most technically complex module, and also the one most frequently underscoped. Your CRM needs to read patient demographics, encounter history, and active care plans from your EHR, and write communication records back. The data standard is HL7 FHIR R4 for modern integrations, with legacy HL7 v2 often required in parallel for older systems.
Multichannel Patient Communication
A unified inbox for SMS, email, and telephony. The architectural requirement is a single system of record for communication history, not separate tools that don’t talk to each other. This matters for continuity of care and for HIPAA audit compliance.
Vick is direct about where this breaks down in practice:
This is a workflow design problem as much as a technology one. A healthcare CRM that routes messages through configurable triage logic, instead of dumping everything into a generic inbox, directly addresses what Vick describes.
Care Coordination and Referral Tracking
For hospital networks and multi-specialty practices, referral management is often the highest-ROI module. This includes tracking outbound referrals, inbound referral conversion rates, and care team coordination workflows for patients with complex or chronic conditions.
Analytics and Reporting
This feature helps measuring patient engagement metrics, communication effectiveness, appointment adherence rates, and referral source attribution. For C-suite buyers, this is often the module that closes the build decision: the ability to see, in one dashboard, what the relationship layer of the organization looks like, and where it’s leaking.
Role-Based Access Control (RBAC) and Audit Logging
It’s not an optional feature but a necessity. Every user in the system has a defined role. Every role has defined permissions. Every access event, read, write, update, delete, gets logged with a timestamp and user ID. This isn’t just compliance architecture; it’s also how you limit blast radius when credentials are compromised.
HIPAA, GDPR & the BAA Question No One Is Asking Their Dev Partner
If you need a quick overview of what matters, here’s a brief HIPAA compliance checklist you can always refer to before signing any vendor:
| # | Compliance Requirement | What to Verify |
|---|---|---|
| PHI encryption at rest | AES-256 encryption applied to all stored patient data | |
| PHI encryption in transit | TLS 1.2 minimum enforced across all data transfers | |
| RBAC configured by clinical role | Access permissions mapped to specific roles — not generic user levels | |
| Audit log covering all PHI access events | Every read, write, update, and delete timestamped with user ID | |
| BAA signed before data access | BAA executed before any developer touches real or production-like patient data | |
| Breach notification procedure documented | Written process in place — who gets notified, in what timeframe, by whom | |
| Data destruction policy at project end | Vendor commits in writing to how PHI is destroyed or returned when engagement closes | |
| Testing environment uses de-identified data only | No real patient records used in dev or QA environments under any circumstances | |
| Penetration testing completed pre-launch | Third-party pen test conducted and findings remediated before go-live |
HIPAA compliance in a healthcare CRM comes down to three things: how you store data, who can access it, and what happens when something goes wrong.
The Storage Requirements Are Well Understood: Encryption at rest (AES-256 is standard), encryption in transit (TLS 1.2 minimum), PHI isolation from non-PHI data, and regular backups with documented retention policies. These are technical requirements your development partner should be implementing as defaults, not as add-ons.
Role-based access is the second layer. Not everyone in a healthcare organization should see everything. A referral coordinator doesn’t need clinical encounter notes. A billing staff member doesn’t need communication history. RBAC ensures that access is scoped to role, that privilege escalation is controlled, and that every access event is logged. The audit log isn’t just a compliance artifact, it’s your forensic record in the event of a breach.
The breach notification requirement is the third layer, and it’s the one that surfaces the question almost nobody asks during vendor selection.
There’s one more area that is often overlooked but carries major significance, it’s the BAA question.
The BAA Question
Under HIPAA, any vendor who stores, processes, or transmits Protected Health Information on your behalf is classified as a Business Associate. That includes your development partner, specifically, any developer who touches real or production-like patient data during build and testing. This legal classification requires a signed Business Associate Agreement before the engagement begins.
A BAA defines the vendor’s obligations around PHI handling: how they store it, who can access it within their organization, what they’ll do if there’s a breach, and how they’ll destroy or return the data at project end.
The problem: many healthcare organizations go through the full vendor selection process, reviewing portfolios, comparing pricing, checking technical capabilities, without ever asking whether the development partner will sign a BAA. And many development vendors who work in healthcare either aren’t clear on the requirement or haven’t standardized the process.
For organizations operating in the EU or handling data from EU-based patients, GDPR adds a parallel layer, a Data Processing Agreement (DPA) is the GDPR equivalent of a BAA. If your patient base includes European residents, you need both.
Healthcare CRM Development Cost in 2026
The range you’ll see everywhere, $40,000 to $300,000-plus, is accurate. It’s also almost useless without context, because the spread is entirely explained by three variables: which EHR integrations you need, what your compliance scope looks like, and how many custom workflows the system needs to support.
If you’re also evaluating costs for other healthcare digital products alongside your CRM, our breakdown of healthcare app development cost covers how these variables shift depending on the product type you’re building.
| Category | MVP ($40K–$80K) | Mid-Market ($80K–$150K) | Enterprise ($150K–$300K+) |
|---|---|---|---|
| What’s included | Core patient data, appointment scheduling, basic multichannel communications, HIPAA architecture, RBAC, audit logging | Everything in MVP + single EHR integration, referral tracking, reporting dashboard, care coordination | Everything in Mid-Market + multiple EHR integrations, full clinical workflow automation, advanced analytics, enterprise RBAC, multi-site architecture |
| What drives cost up | Adding even one EHR integration moves you to the next tier | HL7 v2 support alongside FHIR requires two separate integration architectures | Each major EHR vendor implements FHIR R4 differently, so every integration requires vendor-specific logic |
| Ongoing cost (Year 2+) | $6,000–$12,000/year | $12,000–$20,000/year | $20,000–$35,000/year |
Budget 15–20% of initial build cost annually for security patches, feature iteration, and EHR API updates.
Custom Build vs. Salesforce Health Cloud vs. Off-the-Shelf SaaS: Which Is Right for You?
The cost ranges above assume you’ve already decided to build custom. That’s not always the right call, and committing to the wrong option for the right-sounding reasons is its own category of expensive mistake.
Three viable paths exist. Here’s the quick version, then the reasoning behind it.
| Category | Off-the-Shelf SaaS | Salesforce Health Cloud | Custom Build |
|---|---|---|---|
| Time to launch | 2–8 weeks | 3–6 months | 4–14 months |
| EHR integration depth | Pre-built connectors only | Standard + custom (expensive) | Full, vendor-specific |
| Customization ceiling | Low | Medium | None |
| Data ownership | Vendor-controlled | Vendor-controlled | Full ownership |
| 3-year cost (mid-market) | $60K–$120K | $130K–$220K+ | $100K–$170K |
| Best fit | Standard workflows, smaller teams | Salesforce-native orgs | Unique workflows, deep EHR needs |
Off-the-shelf SaaS
It works if your patient engagement workflows are standard, your team is under 30 users, and you don’t need EHR integration beyond pre-built connectors. These platforms are HIPAA-compliant out of the box, deploy in weeks, and for straightforward use cases, appointment reminders, basic outreach, simple referral tracking, they do the job without a full build. The ceiling arrives when your workflows stop fitting the template. At that point you’re engineering workarounds inside a system not built for them, and that cost compounds quickly.
Salesforce Health Cloud
It is genuinely useful for a specific type of organization: larger health systems already in the Salesforce ecosystem, with complex commercial and clinical workflows running in parallel, and internal admin capacity to configure and maintain it. For everyone else, it tends to be oversold. Licensing runs $300–$600 per user per month. Implementation partners rarely quote below $50,000 for setup alone. For a mid-market clinic group with specific EHR requirements, the three-year total frequently exceeds a purpose-built custom system , without the integration depth that made it worth considering.
Custom Development
It is the right call when your EHR integration requirements go beyond pre-built connectors, your workflows are specific enough that you’d spend significant money bending a platform to fit them, or you need full ownership of your patient data outside a vendor’s data model.
The three-year number matters more than the upfront cost. A $60,000 custom MVP maintained at $15,000 per year lands in roughly the same range as mid-tier Health Cloud licensing for a 20-user team, before implementation and admin overhead. That math shifts by user count, but the gap is consistently smaller than it looks at the point of decision.
If you’re still not sure which path fits, four questions tend to clarify it:
- Do you need bidirectional data sync with your EHR, not just read access?
- Will patients interact directly with the system in ways you need to control and brand?
- Do you have workflows that don’t map to a standard outreach or scheduling model?
- Is your patient data an asset you need to own across vendor relationships?
Two or more yes answers almost always point to custom, whether organizations start there or arrive after a costly detour through the other two.
These are the patterns we’ve seen across every healthcare CRM engagement we’ve scoped. If you want to pressure-test your current plan against them before you commit, → that’s exactly the conversation we start with.
The AppVerticals CRM Scoping Matrix
Before you can pressure-test a vendor quote, you need a framework to sanity-check the number they give you. There are four inputs that determine your realistic cost band:
Input 1: Org type. Telehealth startup, clinic group, multi-specialty practice, hospital network, or digital health product. The org type determines the complexity of workflows, the number of user roles, and the likely EHR environment.
Input 2: EHR integrations required. Zero (manual inputs only), one (the most common), or multiple. Each major EHR integration adds $15,000–$35,000 to scope, depending on the vendor and whether real-time sync is required.
Input 3: Compliance scope. HIPAA only, HIPAA + GDPR, or additional state-level regulations (California CMIA, New York SHIELD Act). Multi-jurisdiction compliance adds audit complexity and affects data architecture decisions made early in the build.
Input 4: Feature tier. MVP (core engagement workflows only), mid-market (EHR integration + referral tracking), or enterprise (full clinical workflow automation + population analytics).
| Org Type | EHR Integrations | Compliance Scope | Feature Tier | Realistic Cost Band |
|---|---|---|---|---|
| Telehealth startup | 0–1 | HIPAA | MVP | $45,000–$75,000 |
| Small clinic group | 1 | HIPAA | Mid-market | $80,000–$120,000 |
| Multi-specialty practice | 1–2 | HIPAA | Mid-market | $110,000–$160,000 |
| Hospital network (regional) | 2–4 | HIPAA + state | Enterprise | $180,000–$300,000+ |
| Digital health product (B2B2C) | 1 | HIPAA + GDPR | Mid-market to enterprise | $120,000–$220,000 |
If a vendor quotes you outside this range without explaining why, ask them to walk through the same four inputs. The right partner can justify every line of their estimate. Muhammad has significantly emphasized on how the type of organization matters most when it comes to calculations in his conversation. He specifically mentioned:
The EHR Integration Reality: What Your Dev Partner Should Tell You before You Sign Anything
EHR integration is the line item that blows healthcare CRM timelines most consistently. Not because it’s technically impossible, but because the time required to get production API access, before a single line of integration code is written, is longer than most project plans account for.
| EHR Vendor | Timeline | Week 1–3 | Week 4–6 | Week 7–10 | Week 11–14+ |
|---|---|---|---|---|---|
| Epic | 6–12+ weeks | MyApp registration | Security review | Technical validation | Health system IT governance → production access |
| Oracle Cerner | 6–10 weeks | Cerner Code application | Documentation review | Technical review | Approval & credentialing → production access |
| Athenahealth | 3–6 weeks | REST API application | Technical review | Approval | Production access granted |
The questions to ask before you sign:
- Have you worked with this specific EHR vendor before? In what context?
- How are you accounting for credentialing time in the project timeline?
- Do you support HL7 v2 alongside FHIR, or FHIR only?
- What happens if EHR vendor approval takes longer than scoped? Is the timeline padded or do we absorb the delay?
A development partner who’s done this before will answer these questions without hesitation. One who’s treating EHR integration as a standard API connection will either sidestep or underestimate them. If your product scope extends beyond CRM, a patient-facing app, a care coordination tool, or a broader digital health platform, our healthcare app development team has handled EHR integration across all major vendors.
Why Healthcare CRM Projects Go Over Budget: The 3 Mistakes We See Repeatedly
Let’s take a detailed look at the areas Muhammad finds as repetitive client mistakes that cause healthcare CRM projects to go over budget:
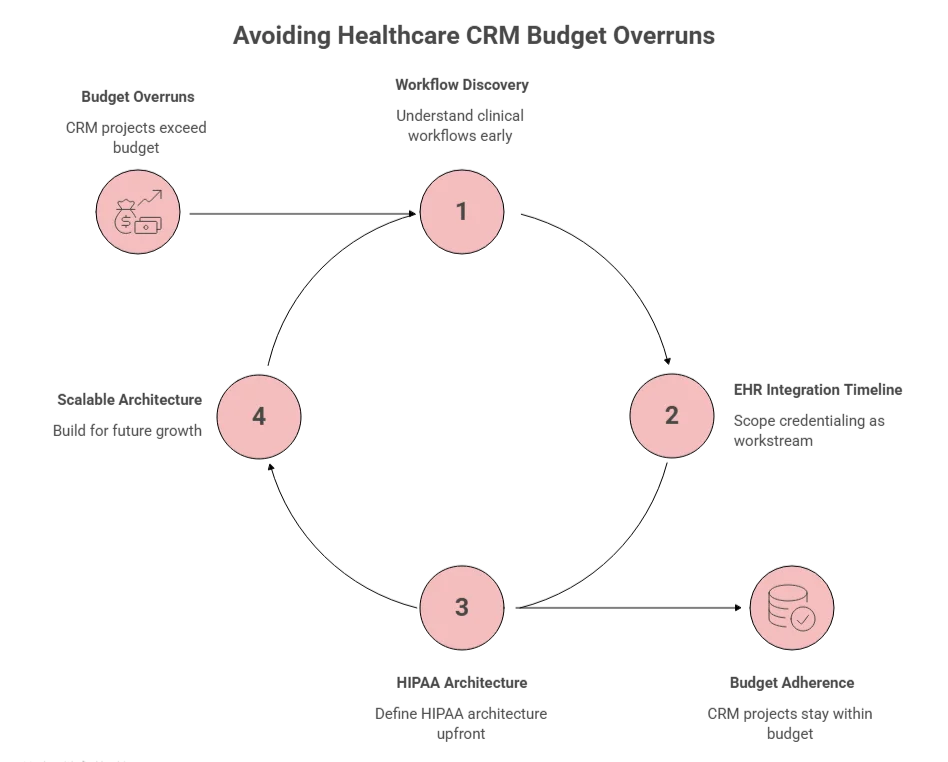
Mistake 1: Treating EHR Integration as a Checkbox, Not a Timeline
The most common budget-blower. A client scopes a 5-month CRM build, allocates 6 weeks for ‘EHR integration,’ and then discovers that Epic credentialing alone takes 10 weeks, before development has started. The project slips. The development team sits partially idle waiting for access. The client pays for the delay.
Muhammad particularly mentioned:
The fix is straightforward: scope the credentialing process as its own workstream at the start of the engagement, run it in parallel with architecture and design work, and build the project timeline assuming the worst-case credentialing window, not the best case.
Mistake 2: Scoping HIPAA Compliance as a Feature, Not a Foundation
HIPAA compliance isn’t a module you add before launch. It’s an architectural decision that shapes everything from the database schema to the deployment infrastructure to the access control model. Muhammad highlights:
The right approach: define the HIPAA architecture before a single line of application code is written. Choose a cloud provider with a HIPAA BAA (AWS, Azure, and GCP all offer them). Structure the data model around PHI boundaries from day one. Implement RBAC and audit logging as foundational components, not add-ons.
Mistake 3: Building for Your Current Org, Not Your Next One
Healthcare organizations change. Practices acquire, merge, and expand. A CRM scoped for 15 users at a single-location clinic looks very different from one that needs to serve 80 users across four locations two years later.
The architecture decisions that govern multi-tenancy, user permission models, and database scaling are made early and are expensive to change later. An MVP doesn’t need to be enterprise-ready on day one, but it does need to be built on a foundation that doesn’t actively prevent scaling. This is a conversation to have before the architecture document is finalized, not after you’ve outgrown a system that wasn’t designed to grow.
How to Choose a Healthcare CRM Development Partner: 5 Questions That Separate the Right Partner from the Rest
Portfolio and price are obvious evaluation criteria but there’s a lot more to consider when choosing your healthcare CRM development partner. These five questions surface what portfolio and price can’t.
- ‘Have you worked with our specific EHR before, and can you show us the integration?’
Not ‘do you have EHR integration experience’, that’s too easy to claim. Specifically: have you integrated with this EHR, what was the scope, and can you walk us through how you handled the credentialing process and the integration architecture?
- ‘Will you sign a Business Associate Agreement before accessing any patient data?’
As covered earlier: this is legally required, not optional. Ask it directly. The response tells you immediately whether the partner understands HIPAA at an operational level or just a theoretical one. If there’s hesitation or confusion, walk away.
- ‘How do you handle compliance architecture, is it built from the start, or scoped as a separate phase?’
The right answer is ‘built from the start.’ Compliance-as-an-afterthought is the single biggest source of healthcare software cost overruns.
- ‘Can you walk us through a project that went over budget or timeline, and what caused it?’
This question doesn’t have a right answer, it has a revealing answer. A partner who can tell you specifically what went wrong, what they learned, and how they’ve changed their process is a partner who has actually shipped healthcare software under real conditions.
- ‘What does your post-launch support model look like?’
Healthcare software doesn’t stop needing attention after launch. EHR vendors update their APIs. HIPAA enforcement priorities shift. Your workflows evolve. You want a defined maintenance agreement, a clear SLA for critical bug fixes, and an explicit plan for handling EHR API updates.
Red flags to watch for:
- Cost estimates delivered without walking through your specific EHR environment and compliance scope
- No healthcare-specific portfolio, or a portfolio that blurs healthcare with general software
- Vague answers about the BAA
- A timeline that doesn’t explicitly account for EHR credentialing
- No dedicated QA process for PHI handling
The Build Decision Carries Consequences That Last Years
A healthcare CRM is not a commodity product. The compliance requirements, the EHR integration complexity, and the variation between org types mean the build decision, what to build, how to scope it, and who you build it with, carries consequences that last years.
Deborah Vick puts the human stakes plainly:
The organizations that get it right treat the development engagement like a clinical system: with documented requirements, a partner who understands the regulatory environment, and clear accountability for every component that touches patient data. The ones that get it wrong typically discover the gap during testing, after the budget is spent.
If you’re scoping a healthcare CRM build, the conversation you need to have is about scope, not just price. That’s where we start.
Ready to build it right?
See how we approach healthcare software development.
View our healthcare software development services





