






















 ChatGPT
ChatGPT
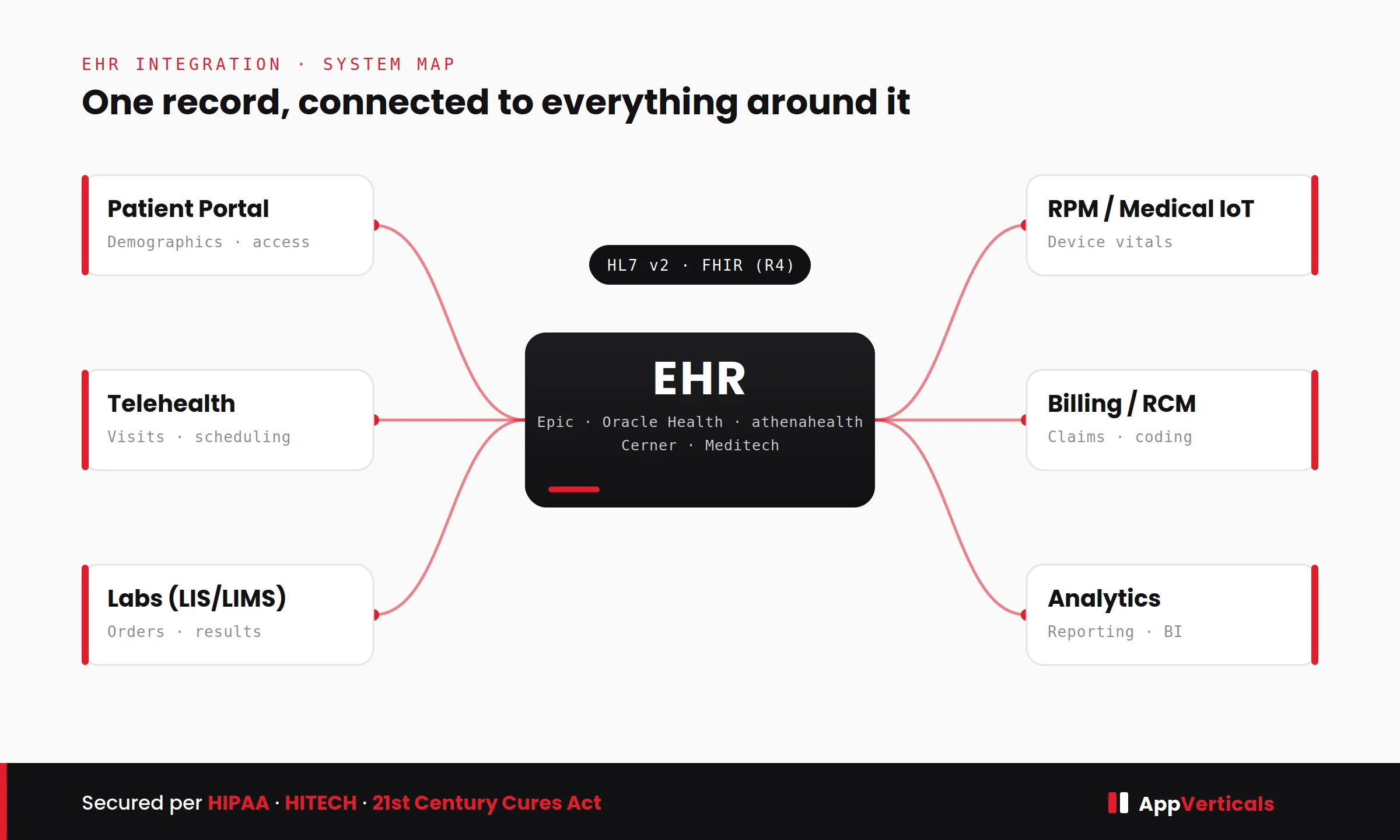
EHR integration is how you get an electronic health record system, Epic, Oracle Health (Cerner), athenahealth, Meditech, and the rest, to talk to the other tools around it, so patient data moves on its own instead of someone re-typing it from one screen into another. That’s the whole game: labs, patient portals, telehealth, and billing, monitoring devices, all reading from and writing to the same record without a human in the middle copying numbers.
I’ve sat in a lot of these conversations from the customer-success side, and by the time someone reaches me they’ve usually stopped asking what integration is. They want the things nobody tells you up front: what it will actually cost, how long it will really take, which technical choices matter, and how to pick a team that won’t quietly burn the budget. So that’s what I want to walk you through here, the way I’d explain it to a client across the table.
Why This Matters More Than It Looks Like It Should
Here’s the thing I wish more teams felt before they felt it the hard way: manual data entry between healthcare systems is slow, and worse, it’s risky. Every time a person re-keys a result or a demographic, there’s a chance of a transposed digit, and every disconnected system is a place where something important can sit unseen. In a clinical setting, that’s not an inconvenience, it’s a safety and compliance problem.
When integration is done right, all of that quiet friction disappears. Results land in the chart automatically, schedules stay in sync, and clinicians spend their time on patients instead of clicking between tabs. And for anyone building a health-tech product, I’d go further: integration is often the difference between a tool people adopt and one they abandon.
I’ve watched it happen. A product that doesn’t connect to the system clinicians already live in all day is a product they’ll quietly stop opening. It doesn’t matter how good the idea is. Treat integration as a feature to bolt on later and you’ve already lost; it’s the thing that decides whether anyone actually uses what you built.
HL7 or FHIR? The Choice That Quietly Shapes Everything
Almost every integration I’ve been part of comes down to two standards, and you don’t need to be an engineer to understand the trade-off.
HL7 v2 is the older one. It’s been moving clinical data for decades, it’s everywhere, and it’s proven, it’s not going anywhere. FHIR is the modern approach, built on the same kind of web technology that powers most apps you use every day. It’s what regulators now lean toward and what most new builds start with, because it’s cleaner to connect and cheaper to maintain over time.
When someone says “the API,” they almost always mean FHIR, most major EHRs offer one now. The catch I always flag for clients is that FHIR coverage is uneven. A vendor might hand you patient details and lab results through FHIR but still make you use the older HL7 method for something like certain scheduling data. That’s why, in practice, the answer is rarely one or the other.
The momentum is clearly with FHIR, though, and it’s part of a wider shift I keep seeing across the industry, if you want the broader view, we’ve written separately about the latest healthcare software development trends, and interoperability sits right at the center of them.
A Simple Way to Decide: HL7 V2 Or FHIR?
Lean FHIR when: you’re building something new, you need to meet patient-access compliance rules, you want lower upkeep down the road, or you’re connecting modern cloud apps.
Lean HL7 v2 when: you’re plugging into older interfaces that already exist, or the specific data you need isn’t available through FHIR yet.
If you want to see how we map each of these to a specific use case, that’s the core of our interoperability & EHR integration services.
How the Data Actually Travels
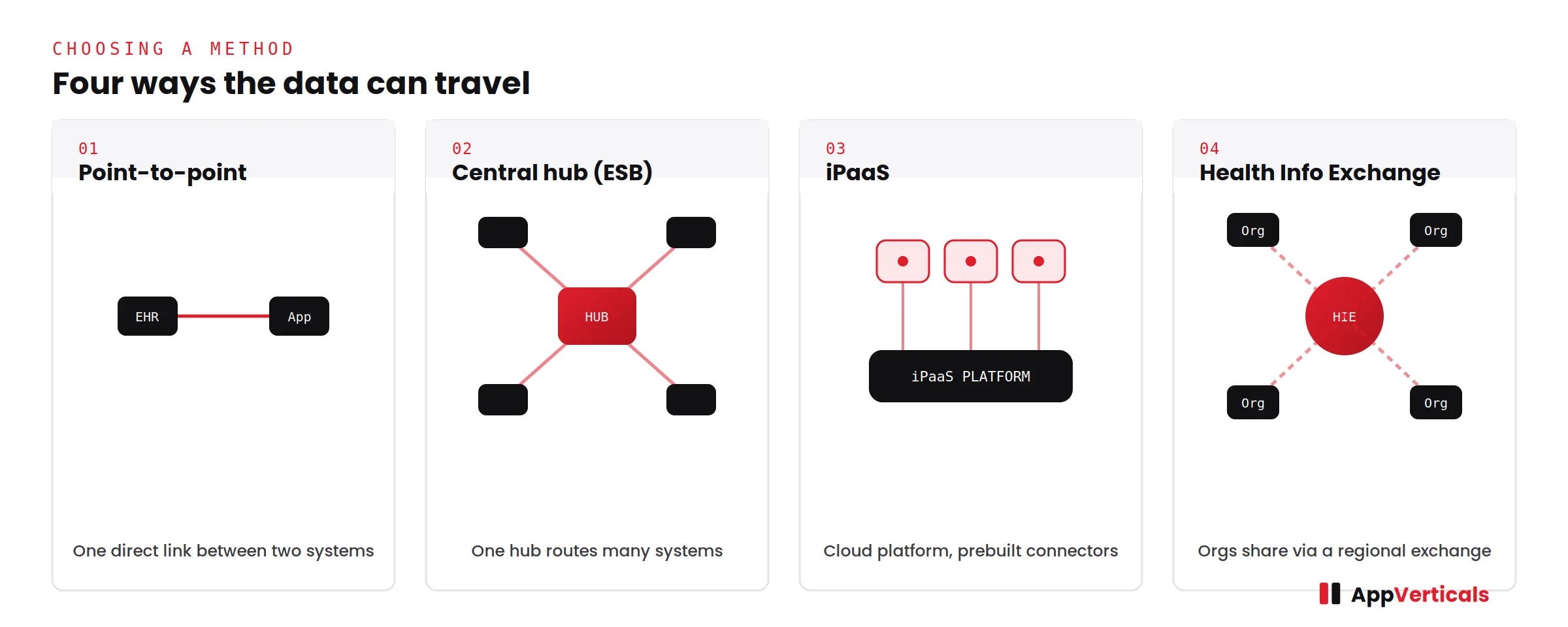
Choosing a standard decides how the data is formatted. The next choice is how it travels, and the right answer depends almost entirely on how many systems you’re connecting now and how many you’ll add later.
| Approach | What it is, in plain terms | Best for | The catch |
|---|---|---|---|
| Point-to-point | A direct line between two systems | One connection that won’t grow | Gets messy and expensive once you add more systems |
| Central hub (ESB) | One hub routes messages between many systems | Hospitals with lots of internal connections | More work to set up and maintain |
| iPaaS | A cloud platform with ready-made connectors | Teams who want a faster, managed setup | Less custom control; ongoing platform fee |
| Through an exchange (HIE) | Connecting via a regional health data exchange | Sharing data across organizations | Depends on what that exchange supports |
What EHR Integration Actually Costs In 2026
This is the question almost everyone arrives with, so let me give you real numbers instead of “it depends.” The ranges below are the bands we genuinely work within for compliant delivery, and they hold up well against current market pricing.
| What you’re building | Typical cost | What to know |
|---|---|---|
| Pull data in from one EHR, a couple of data types (FHIR) | $15K – $30K | The cheapest way in; the wait for sandbox approval sets the timeline |
| Two-way connection with one major EHR (Epic / Cerner) | $40K – $80K | Epic’s certification process adds cost and time |
| Full two-way suite (FHIR + HL7 v2 via middleware) | $50K – $80K per platform | Covers clinical data, orders, results, scheduling, meds |
| Multiple EHRs connected at once | $100K – $150K+ | Each system needs its own testing and IT coordination |
| Ongoing upkeep (per connection, per year) | $3K – $15K | Monitoring, fixing issues, keeping up with vendor changes |
When I explain why one project costs three times another, it always comes back to four things: which direction the data flows (pulling data in is far cheaper than full two-way sync), which standard you use, how many types of data you’re moving (demographics is one thing; orders, results, scheduling, and medications each add work), and which EHR you’re connecting to, more on that next.
And here’s the part I push hardest on with clients, because it’s where budgets quietly leak: the expensive surprises are almost never the code. They’re the things outside our control, waiting on a vendor’s sandbox approval, sitting in a certification queue, or stuck behind a hospital’s own IT backlog.
He’s watched the technical build finish quickly only for the timeline to stretch because of vendor onboarding, security reviews, and testing sign-offs the development team never controlled. So if a partner quotes you a number without warning you about any of that, the number isn’t real yet.
And if integration is one piece of a larger build, it’s worth looking at the full picture of healthcare app development costs so the integration budget sits in context rather than in isolation.
The Vendor You Connect To Changes the Math
The single biggest thing teams underestimate is which EHR is on the other end. It’s tempting to think of “the EHR” as one generic thing, but the vendor sets a huge share of your cost and timeline before we write any code.
| EHR System | Relative Effort | Typical Cost (Single-Vendor Integration) | Why |
|---|---|---|---|
| athenahealth | Lowest | $15K – $45K | Built cloud-first and API-friendly; least friction to connect |
| Epic | Highest | $50K – $100K+ | Requires certification and approval process before integration |
| Oracle Health (Cerner) | Mid–High | $45K – $90K | Powerful system, but compliance and approval cycles extend timelines |
| Meditech / Allscripts | Depends on the site | $40K – $85K | Variability across deployments; features differ by hospital setup |
How Long Does EHR Integration Take?
Timelines follow scope closely, and just like cost, most of the variation comes from waiting on other people rather than from the engineering itself.
| What you’re building | Typical timeline | What sets the pace |
|---|---|---|
| Pulling data in from one EHR | 4 – 6 weeks | Waiting on sandbox approval |
| Two-way connection with Epic / Cerner | 10 – 14 weeks | The certification process |
| Multiple EHRs in production | 16 – 24 weeks | Testing each system + each hospital’s IT queue |
Notice the pattern. Pulling data in from one system is usually a four-to-six-week job. A two-way Epic or Cerner connection runs ten to fourteen. Connecting several EHRs at once is a sixteen-to-twenty-four-week effort. But the long poles holding up almost every one of these are approvals, certification, and someone else’s IT queue, not the time it takes us to write the code.
What Does the EHR Integration Process Actually Look Like?
Whenever a client asks how we’ll run the project, I describe six stages. None of this is mysterious, it’s just disciplined.
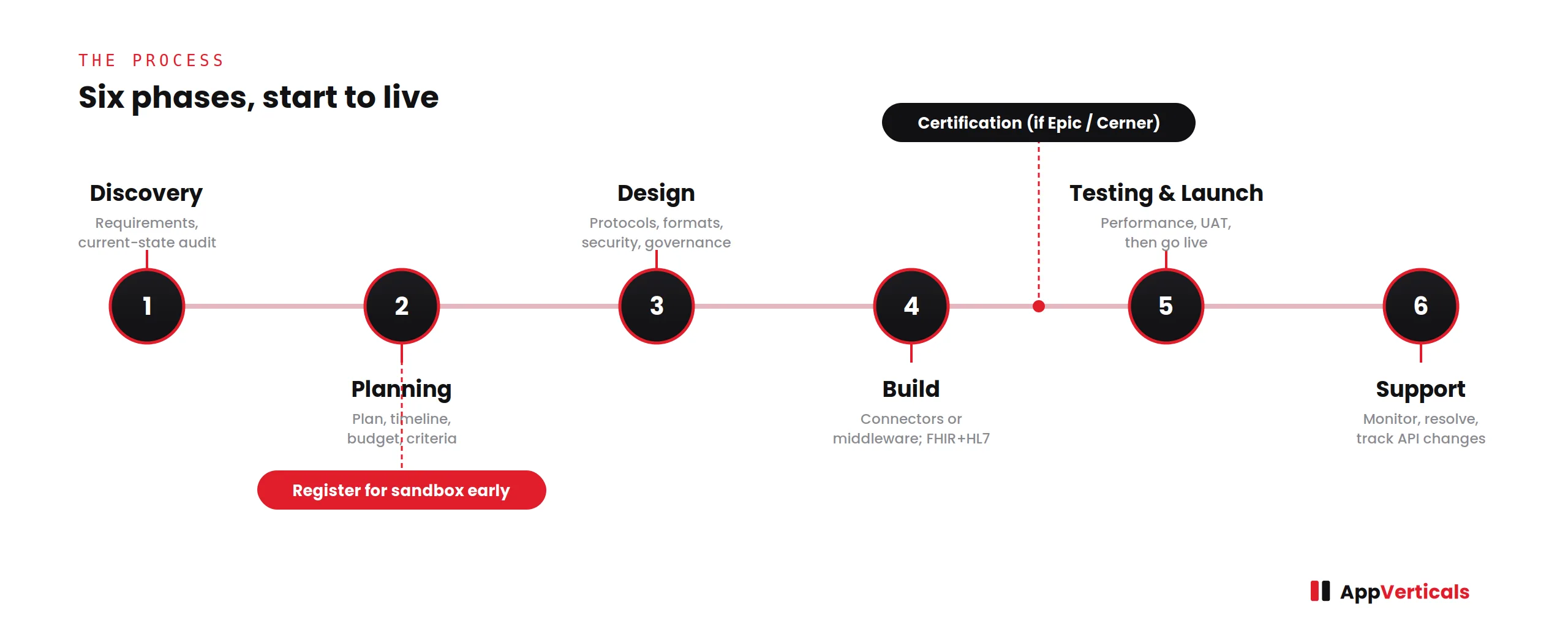
- Discovery: We gather requirements, look at your current systems, and settle the technical choices: which standard, which method, which data. Getting this right is what keeps everything later from ballooning.
- Planning: We lock the plan, timeline, budget, and what “done” means. And critically, we register for the EHR’s sandbox immediately, since that approval is often the longest wait, starting it early is the cheapest time you’ll ever save.
- Design: We define how systems will communicate and, just as importantly, how we’ll keep the data secure and compliant. This is where HIPAA gets built in from the start rather than bolted on at the end.
- Build: We create the connections or set up the middleware that links your EHR to the other system. For hybrid projects, this is usually where the FHIR and HL7 pieces get wired together.
- Testing and launch: We test for performance, security, and real-world use, fix what breaks, then go live and train your team. With clinical data, there’s no “we’ll test it in production.”
- Support: We keep an eye on it, resolve issues, and stay ahead of the vendor’s own updates. An integration nobody maintains slowly falls apart.
The Most Expensive Integration Mistake I See Clients Make
Most of the pain in these projects is predictable, which is the good news, predictable means avoidable.
That last one is the mistake I spend the most energy heading off. Teams ask for two-way sync because it sounds complete and thorough. But honestly, half the time they only ever needed to pull data in. That one assumption can double or triple the budget and add months of certification they never needed.
Arif framed it better than I usually do. The common version he sees is a client wanting full bi-directional integration with multiple EHRs from day one, when their actual business need could be met with a simpler phased rollout. As he put it:
So the first thing I do with every client is help them separate what they truly need right now from what merely sounds impressive. Start with the workflows that move the needle, prove adoption, and then expand.
The fix isn’t glamorous, but it works every time: write down exactly which data you need and which direction it has to move, check each one against a real workflow, and get your sandbox access started on day one.
A Custom ERP Built by AppVerticals
At the end of the day, all of this is really about one thing, keeping patient data secure, compliant, and connected while it moves through a real care workflow. The projects I’m proudest of are the ones where we got that right from the ground up.
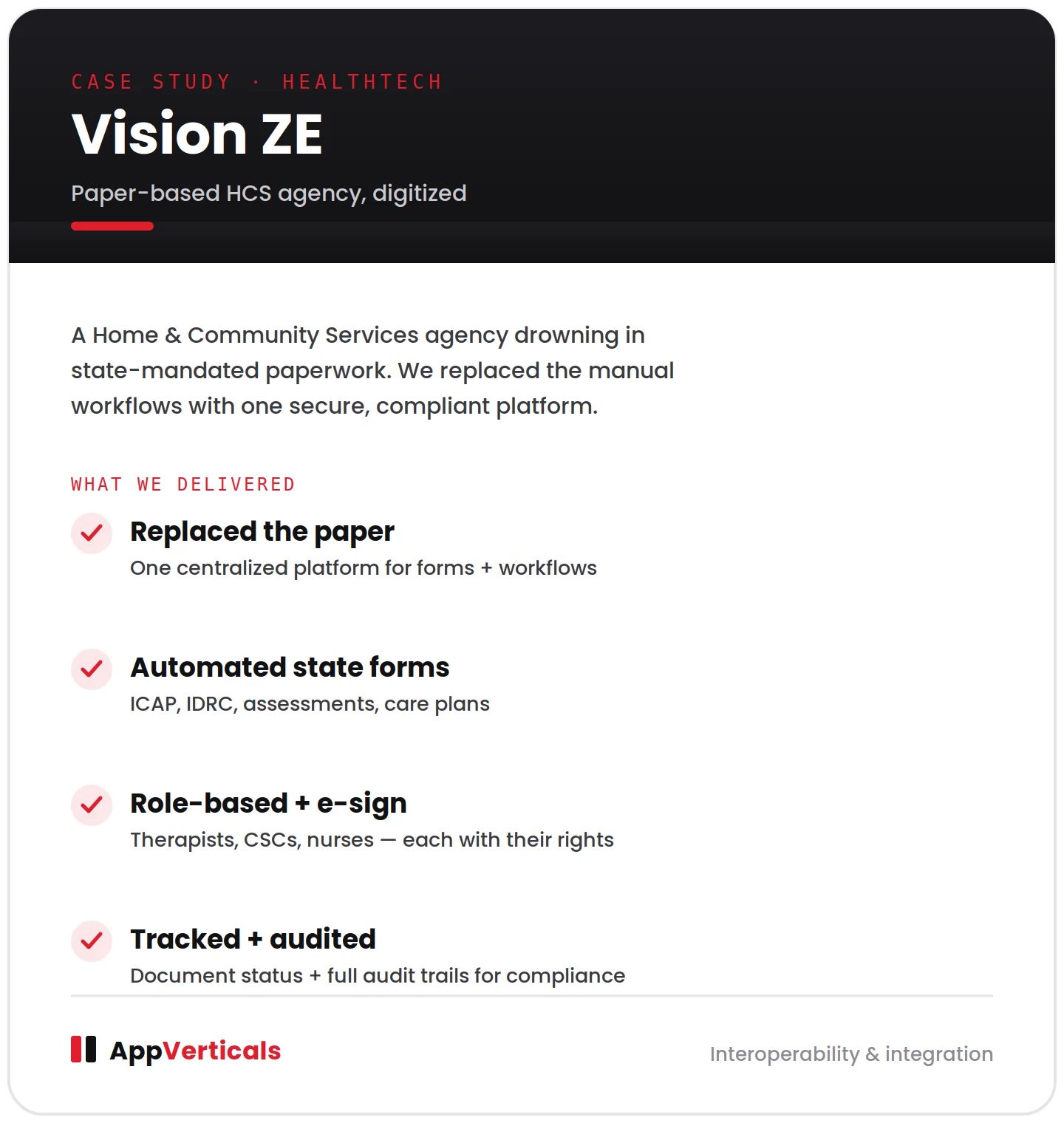
One I point to often is Vision ZE. They run a Home and Community Services (HCS) agency, and they came to us to modernize operations that still leaned heavily on paper documentation and manual workflows. If you know the HCS world, you know the weight of it: every consumer comes with a stack of state-mandated forms, ICAP, IDRC, assessments, care plans, compliance documents, and each one has to be completed by a specific role, whether that’s a therapist, a client service coordinator, or a nurse, then routed through its own approval and signature rules.
Doing that on paper is slow and risky. Forms get lost, compliance gets tracked by hand, and nobody has a clear view of what’s been signed and what’s still outstanding. So we built them a centralized digital platform that replaced the paper, automated those workflows, enforced role-based permissions, handled electronic signatures, tracked the status of every document, and kept a full audit trail — all aligned to agency and state requirements.
The reason I bring up an agency-forms project here is that the hard part is identical.
Build It Yourself, Buy It, or Bring In A Partner
There are really three ways to get an integration done, plus a fourth option I think people should hear more often.
Building it in-house makes sense if you already have engineers who know healthcare interoperability and you’ll be maintaining lots of these over time.
Buying, using a vendor’s ready-made connectors or a platform with templates, is fastest when your needs line up neatly with what’s available off the shelf.
Bringing in a partner is the right call when you want production-grade, compliant work without standing up a permanent integration team, especially anything involving Epic, where having shipped against that exact system before saves real money.
And the fourth option I’ll always name honestly: sometimes you don’t need a custom integration at all. For a small practice, a full custom build can mean weeks of IT tickets and coordination they don’t have the appetite for.
Lighter tools, vendor connectors, ready-made templates, or newer products that push data straight into browser-based records, may get you where you need to go faster and cheaper. Match the effort to your scope, and only pay for custom work when the simpler options genuinely fall short.
If you’re weighing this across a bigger product roadmap, our healthcare software development services cover more than a single connection. And if a CRM is one of the systems you’re planning to wire into the EHR, which it often is, once billing and patient outreach enter the picture, our healthcare CRM software guide is a good place to think that part through.
How to Choose Your EHR Integration Partner?
By the time you’re comparing partners, the technical questions matter less than the track-record ones. Here’s the short list I’d use myself:
- Have they actually shipped against your EHR? Especially with Epic, ask for it directly, because that experience doesn’t transfer from a generic résumé.
- Do they bring up security on their own? A serious partner talks about agreements, encryption, access controls, and audit trails before you have to ask.
- Will they talk you out of work you don’t need? The right team should be willing to tell you two-way sync is overkill for your case.
- Do they quote the waiting, not just the building? Approvals, certification, and IT queues should all be in the estimate.
- Can they show real, compliant healthcare work? That mindset matters far more than headcount.
Conclusion
The real decision in front of you was always how to integrate, not whether: which standard, which method, whether to build or partner, and at a cost and timeline you can stand behind. A simple connection can be live in six weeks for the price of a mid-size feature. A multi-system, Epic-certified setup is a six-figure, multi-quarter commitment. The teams that stay on budget are the ones that scope honestly up front and bring in people who’ve already done it against that exact system.
If you’re weighing your options, that’s the whole range we cover, from a single connection to a multi-system rollout and we’re happy to help you figure out what actually fits your scope.
Scope your EHR integration with people who've shipped it before
From a single FHIR connection to a full multi-system rollout, see exactly how we approach interoperability, standards, methods, compliance, and all.
Or if you need a rough estimate only, our app cost calculator can help!






